


What's the Deal with CMS Direct Contracting?
It's actually kind of a big deal

One of the key things I’ve learned during my time working in healthcare is that some of the biggest changes and opportunities come from the U.S. government.
For example, the Affordable Care Act of 2009 resulted in providers starting to be measured for their health outcomes and readmissions. This led to the creation of a whole new crop of healthcare startups (including one I worked at in the past - shoutout to CipherHealth) that helped providers measure better measure these outcomes and improve them.
While not at quite the same magnitude as the ACA, I do feel that CMS Direct Contracting represents a similar opportunity for innovation for both primary care providers (PCPs) and entrepreneurs.
But First, What Is It?
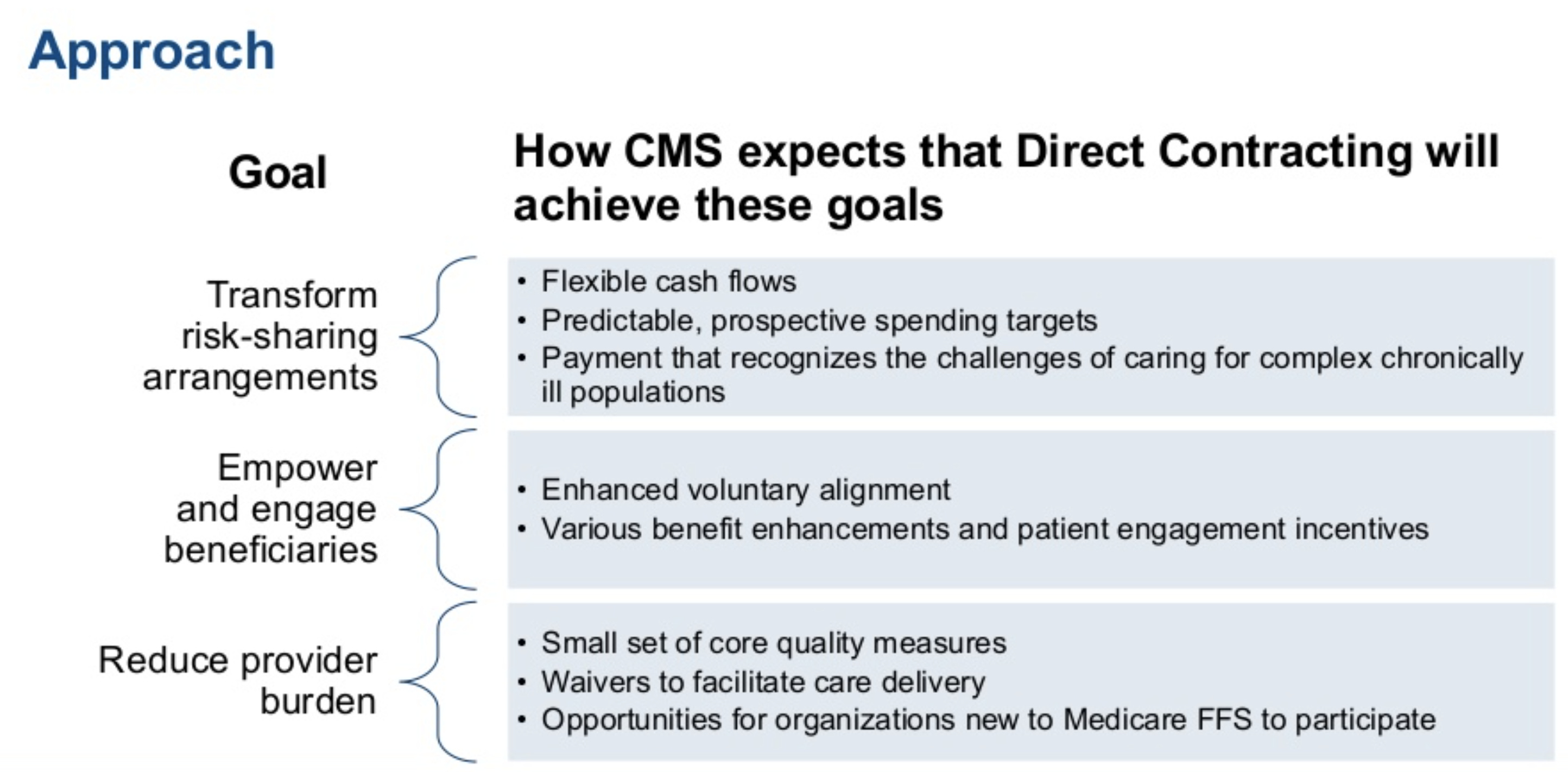
I won’t fully reiterate what CMS has already laboriously written about in detail here, but the Direct Contracting Model has three goals:

It seems like CMS is continuing to double-down on the need to move towards value-based reimbursement models, while also recognizing that their efforts won’t be effective if they make it too difficult for providers to participate.
The Direct Contracting Model provides multiple strategies for addressing each of these goals:
The key idea is that Direct Contracting would be a capitated model, where CMS would pay each participating primary care provider a fixed amount to take care of a patient for a certain period of time in advance, and allow the PCPs to share in the upside and downside risk.
The other key point is that CMS has called out this approach is meant to “reduce provider burden” through a reduced set of quality measures, which I think will be a plus for engagement. I believe this is a beneficial development from the earlier phases of value-based contracting, which placed too much of a reporting burden on providers.
Most importantly, provider organizations that become Direct Contracting Entities (DCEs) will be able to choose which level of risk (both upside and downside) they want to take on on a spectrum:

It will be interesting to see data on how many DCEs ended up applying this year (the deadline closed in July) and which Risk Options they chose to pursue. My instinct is that most DCEs will start on the lower-risk side (Professional) of having 50% upside/downside, since even that will be big shift compared to how they were paid previously.
Why Direct Contracting Matters
The rollout of the Direct Contracting program seems important for a few reasons:
It gives PCPs that are contracted with Medicare FFS a way to participate directly in value-based contracts with (hopefully) reduced reporting burdens. I hope that this approach will give PCPs more freedom and economic incentives to actually spend time practicing good preventative medicine, as opposed to just trying to meet the quotas that the current FFS system incentivizes economically.
It is a model that allows for 100% risk-sharing of upside/downside, which I haven’t seen yet. I believe that this better aligns the incentives of the payor, patient, and provider from an economic perspective.
It shows that CMS is committed to shifting more-and-more reimbursement towards value-based models, a precedent that private payors will continue to take note of.
Opportunities
I see a few immediate opportunities:
PCPs who want to practice medicine at a more sustainable pace and who want to focus on prevention may choose to switch to practices or DCEs that operate under this model
Healthcare technology companies may shift more of their business model to focus on products that support primary care providers and preventative strategies under a Direct Contracting model, capturing a bit of the upside value
New generation “tech-forward” providers (think One Medical) will be able to make a faster transition to this payment model and potentially gain market share in the Medicare arena.
I’m excited to see how this develops!
What opportunities are you seeing as a result of Direct Contracting? Thoughts, tips, articles appreciated!
Alex
twitter: @ayliu22
Like this article? Share or subscribe for in-depth pieces on digital health and the future of healthcare below: